According to the American Heart Association, congenital heart defects (present at birth) are the most common type of birth defect. They affect 8 out of every 1,000 newborns. Each year, more than 35,000 babies in the United States are born with congenital heart defects.
Although the condition is rare, Tetralogy of Fallot (TOF) is the most common congenital (present at birth) heart defect causing a “blue baby.” According to the National Heart, Lung, and Blood Institute (NHLBI), TOF affects roughly 5 out of every 10,000 babies. The defect is found equally among boys and girls.

TOF usually is diagnosed based on the above signs and symptoms, a physical exam, and the results from tests and procedures. During a physical exam, your doctor will listen to your baby’s heart and lungs to check for a murmur and will evaluate your baby’s general appearance to look for signs of a heart defect, such as a bluish tint to the skin, lips, or fingernails and rapid breathing.
If your doctor finds any signs of TOF, your baby likely will undergo additional testing. Tests that your doctor may order include a chest x-ray, echocardiogram (echo), electrocardiogram (EKG), pulse oximetry, or cardiac catheterization. For more information on these tests, visit our common diagnostic tests page.
The only treatment for TOF is open heart surgery.
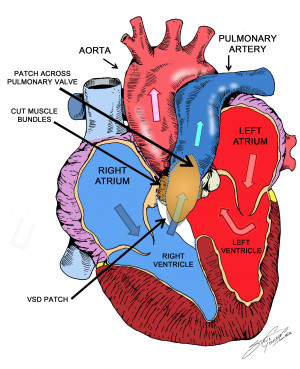
Illustration of a heart with a repaired VSD. Illustration by Steven P. Goldberg, MD
Timing of treatment varies, but the more common approach is to wait until your child is about 3-6 months old.
Some babies with TOF can have very low blood oxygen levels soon after birth. If your baby is too weak or too small to have full repair at this stage, the surgeon may perform an initial surgery (shunt procedure) to help increase blood flow to the lungs and give him or her time to grow and get strong enough for the full repair. Complete corrective surgery is done later in life.
Be sure to speak with your baby’s doctor about what you should expect during and after the surgery. You can print these sample questions to use as a basis for discussion with the doctor.
Expected outcomes: The Society of Thoracic Surgeons (STS) Congenital Heart Surgery Database shows an expected outcome of 1.1% mortality for isolated Tetralogy of Fallot. Outcomes will vary across different programs. It is appropriate to inquire about the outcomes of a surgical group or surgeon during your consultation.
Without surgery, TOF can be fatal and most people die by age 20.
After surgery, your baby will require continued follow-up care. The doctor will schedule routine checkups to make sure that the procedure was successful and monitor for any new problems.

Most children with successful complete repair will not have any activity restrictions as they grow older.
Sometimes, patients who had an operation to repair TOF in childhood need additional surgery as they age. Most often, this procedure is undertaken to reduce leakage of blood back into the right ventricle, and more frequently is required in children whose native pulmonary valve was not usable at the time of the initial repair.
Your child may be required to take antibiotics during dental procedures to prevent infections that may cause inflammation of the heart (endocarditis). Preventive antibiotics are almost always recommended for people who have artificial valves or who’ve had repair with prosthetic material. Be sure to ask your doctor about what is right for your child.

Reviewed by: Ram Kumar Subramanyan, MD, PhD
December 2017
The STS mission is to advance cardiothoracic surgeons’ delivery of the highest quality patient care through collaboration, education, research, and advocacy.