Mitral valve disease occurs when the mitral valve doesn’t work properly.
There are two main types of mitral valve disease:
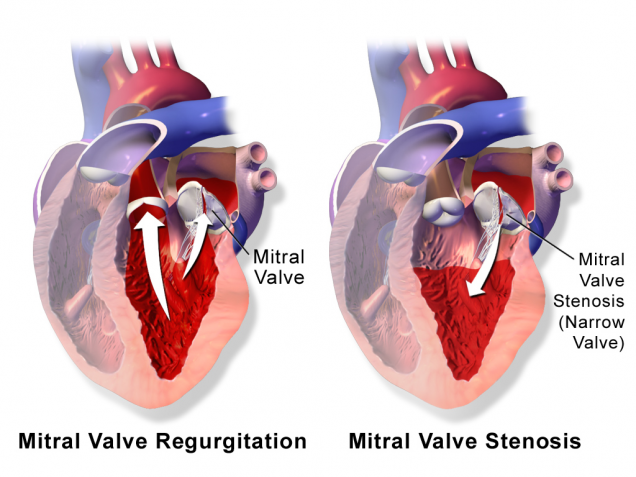
- Stenosis – the valve does not open enough to allow sufficient blood flow. Usually this is the result of hardening (calcification) of the leaflets, which prevents their movement.
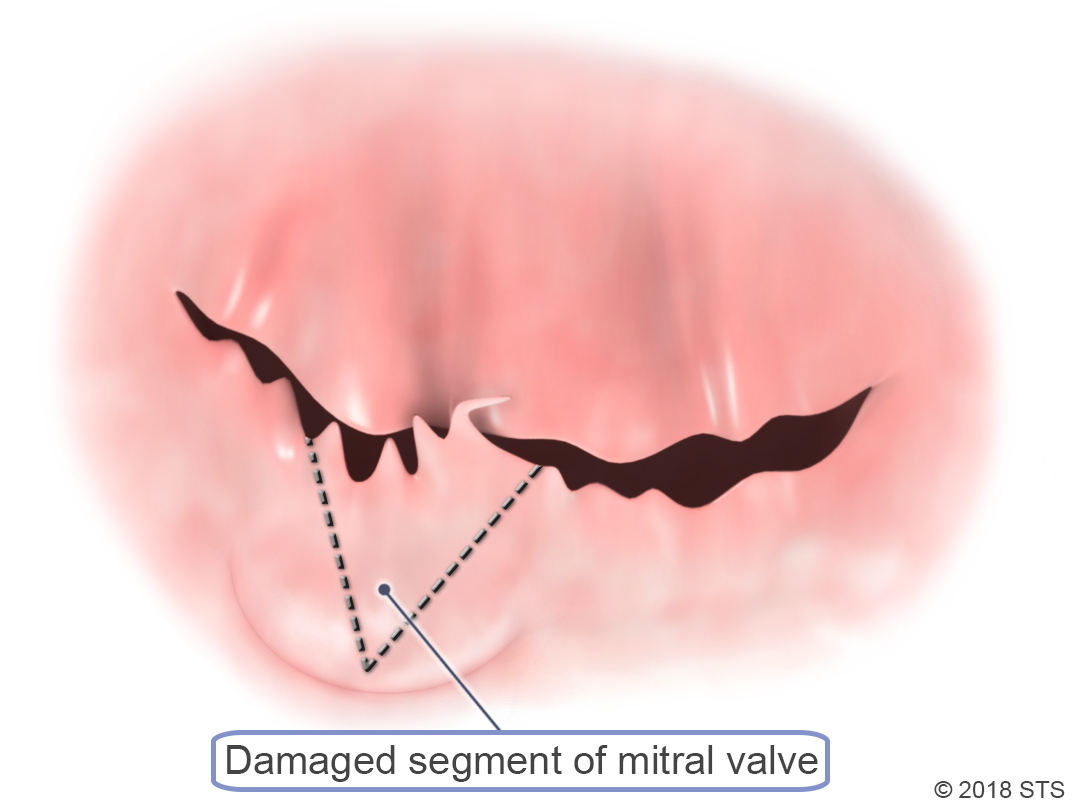
- Regurgitation – blood leaks backward out of the valve. Usually this is either the result of the leaflets being pulled apart so that blood leaks backward between them, or by damage to the valve structure.
Your doctor can usually diagnose mitral valve disease based on your medical history, risk factors, a physical exam, and results from tests and procedures.
There is no one test that can diagnose mitral valve disease, so your doctor may recommend one or more of the following: electrocardiogram (EKG), echocardiogram (echo), chest x-ray, blood tests, and coronary angiography. For more information on these tests, visit the common diagnostic tests page.
A faulty mitral valve that is not causing symptoms may not need any treatment, and mild symptoms may be treated with medication. With more severe symptoms, surgery may be required.
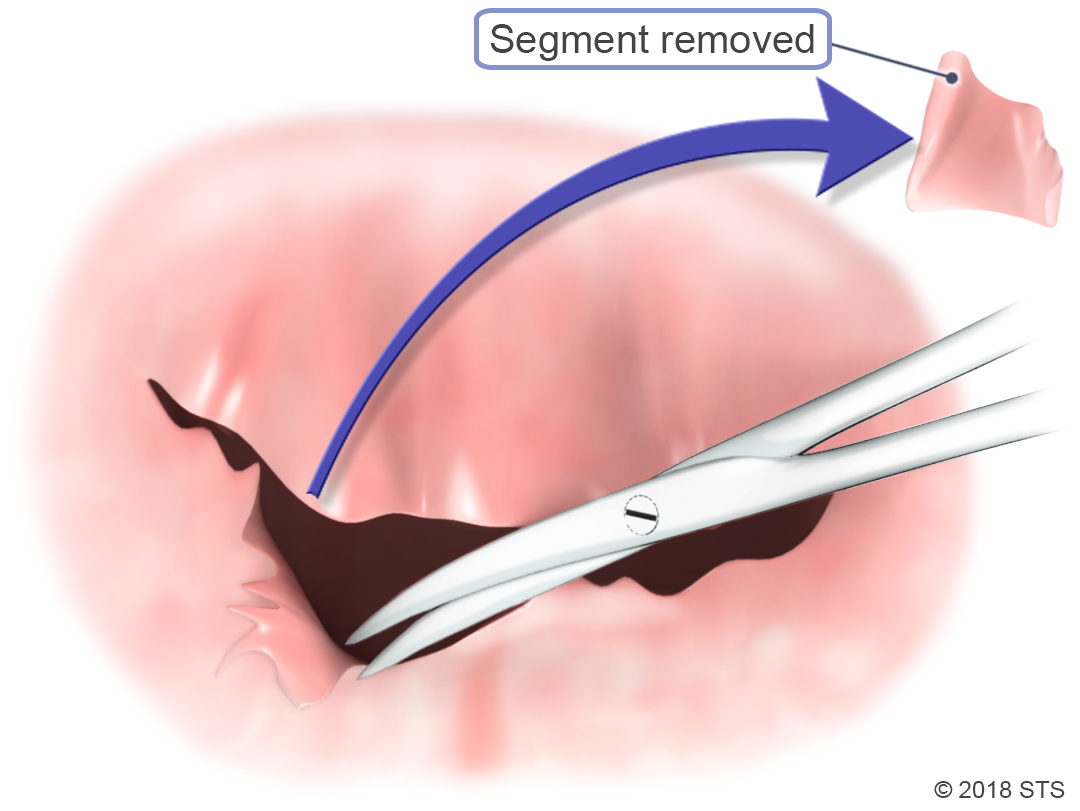
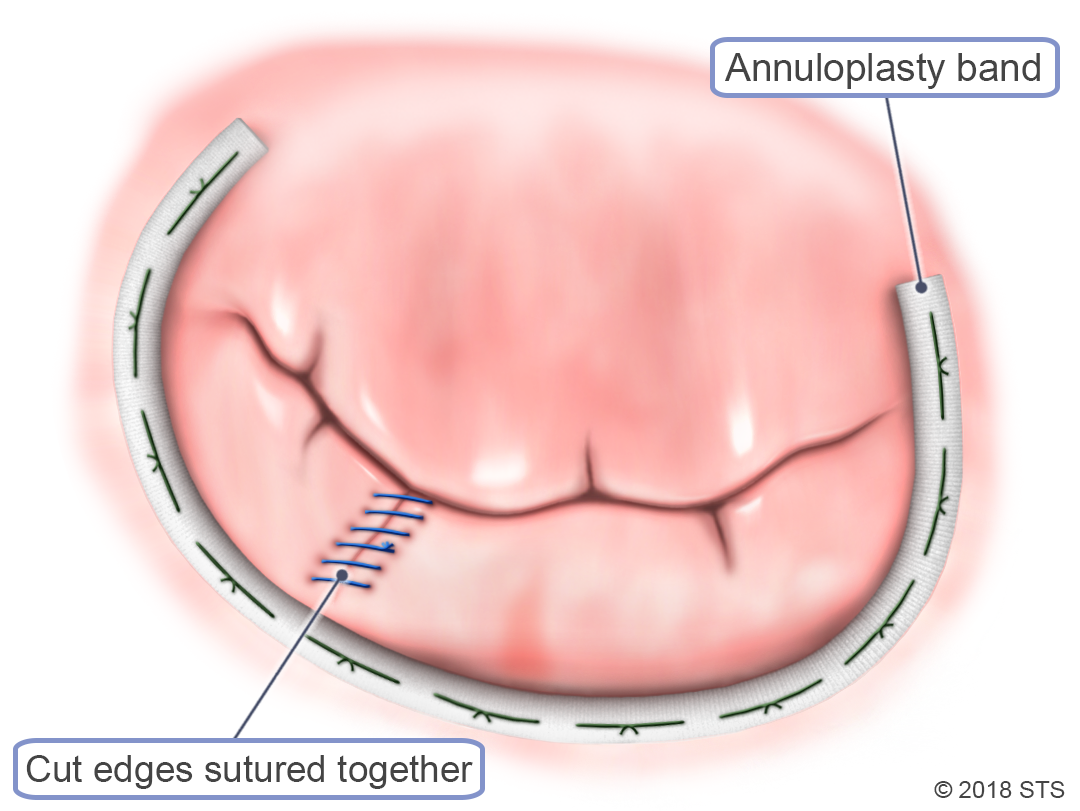
Doctors will often repair the mitral valve when possible, but replacement is sometimes necessary.
Together with you and your medical team, your doctor will determine the best treatment option based on your symptoms and test results. You can print these sample questions to use as a basis for discussion with your doctor or a cardiothoracic surgeon.
You also can access the STS Risk Calculator, which can help calculate your risk of death or other complications from certain types of heart surgery. The results can help you and your doctor to determine the best course of treatment.

Reviewed by: Robbin G. Cohen, MD, with assistance from John Hallsten and Travis Schwartz
July 2016
Previously reviewed by: Emily A. Farkas, MD and Fernando Fleischman, MD
The STS mission is to advance cardiothoracic surgeons’ delivery of the highest quality patient care through collaboration, education, research, and advocacy.