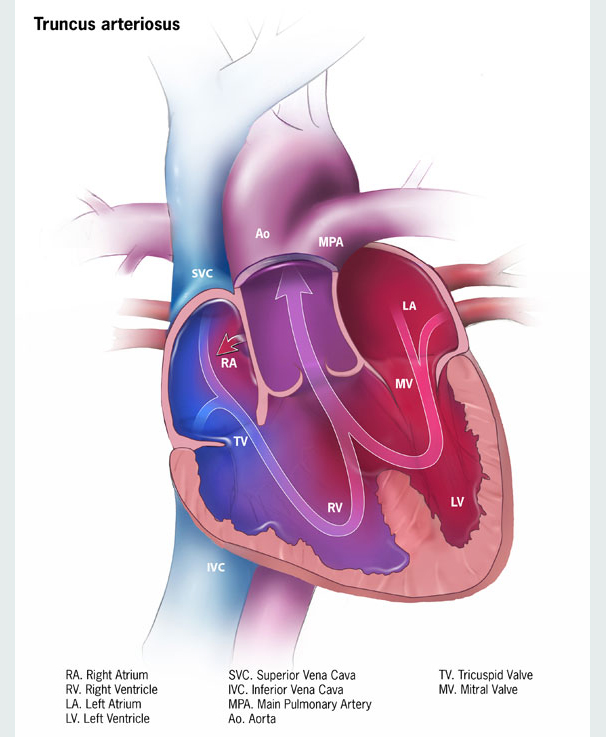
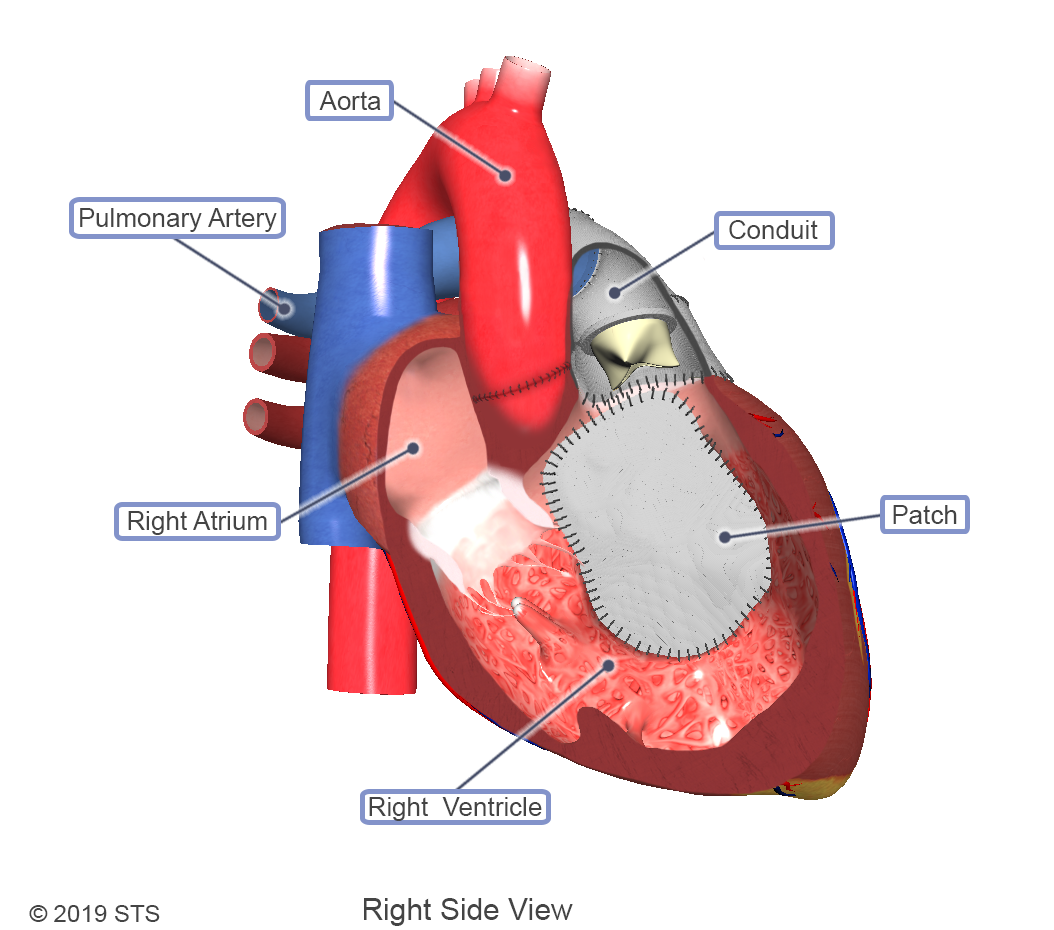
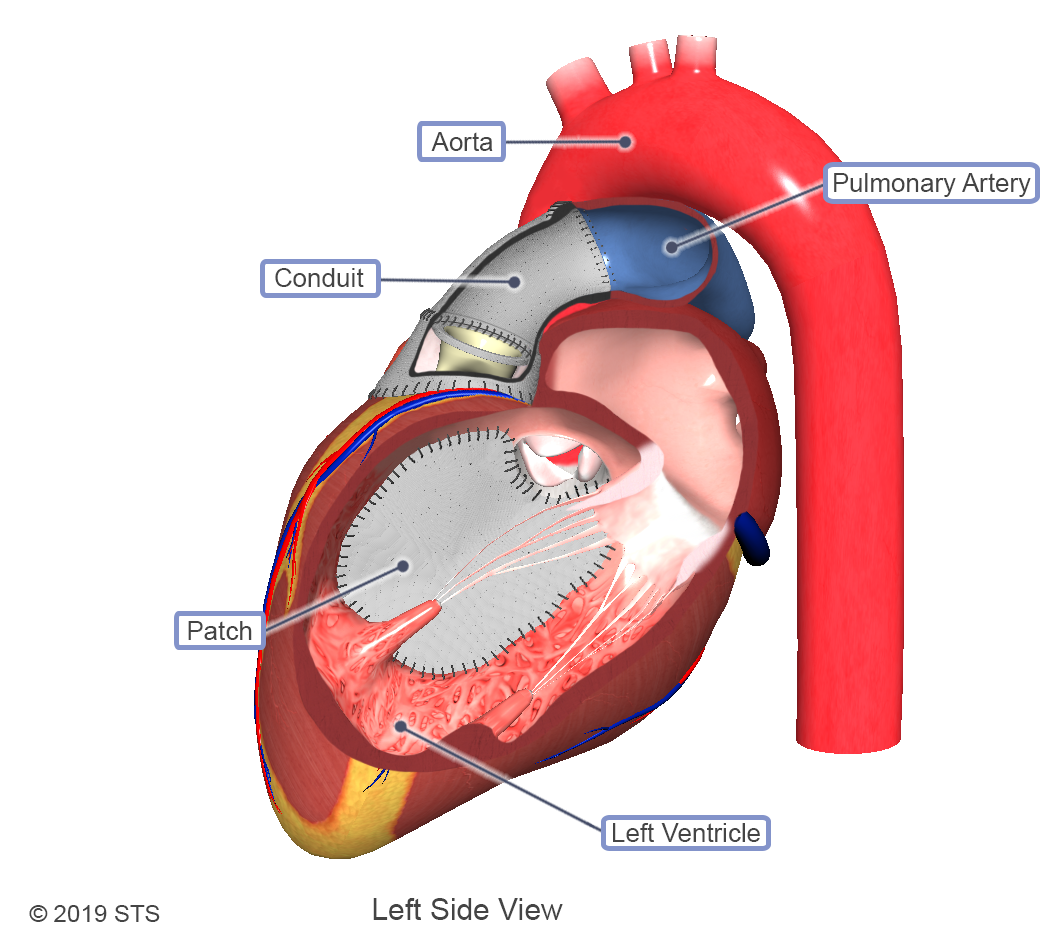
Cases of truncus arteriosus can vary depending on how the pulmonary arteries exit the aorta. Along with the different types, varying levels of complexity exist within this one diagnosis. With truncus arteriosus, a large hole is usually found between the two ventricles (ventricular septal defect), which causes oxygen-poor (blue) blood and oxygen-rich (red) blood to mix together; too much blood goes to the lungs, and the heart works harder to pump blood to the rest of the body.
The truncal valve is often abnormal with this disease. It can be thickened and narrowed, which can block the blood as it leaves the heart, or it can leak, causing blood that leaves the heart to leak back into the heart across the valve. The presence of narrowing and leaking is a predictor of poorer outcomes.
According to the Centers for Disease Control and Prevention (CDC), truncus arteriosus occurs in fewer than one out of every 10,000 live births, which means that about 300 babies are born with truncus arteriosus each year in the United States.
In most cases this one test will provide enough evidence to recommend treatment, but in rare occasions your baby may undergo a cardiac catheterization for further analysis.
Other tests your doctor might order to confirm a diagnosis include chest x-ray, electrocardiogram (EKG), or magnetic resonance imaging (MRI).

For more information on these tests, visit our common diagnostic tests page.
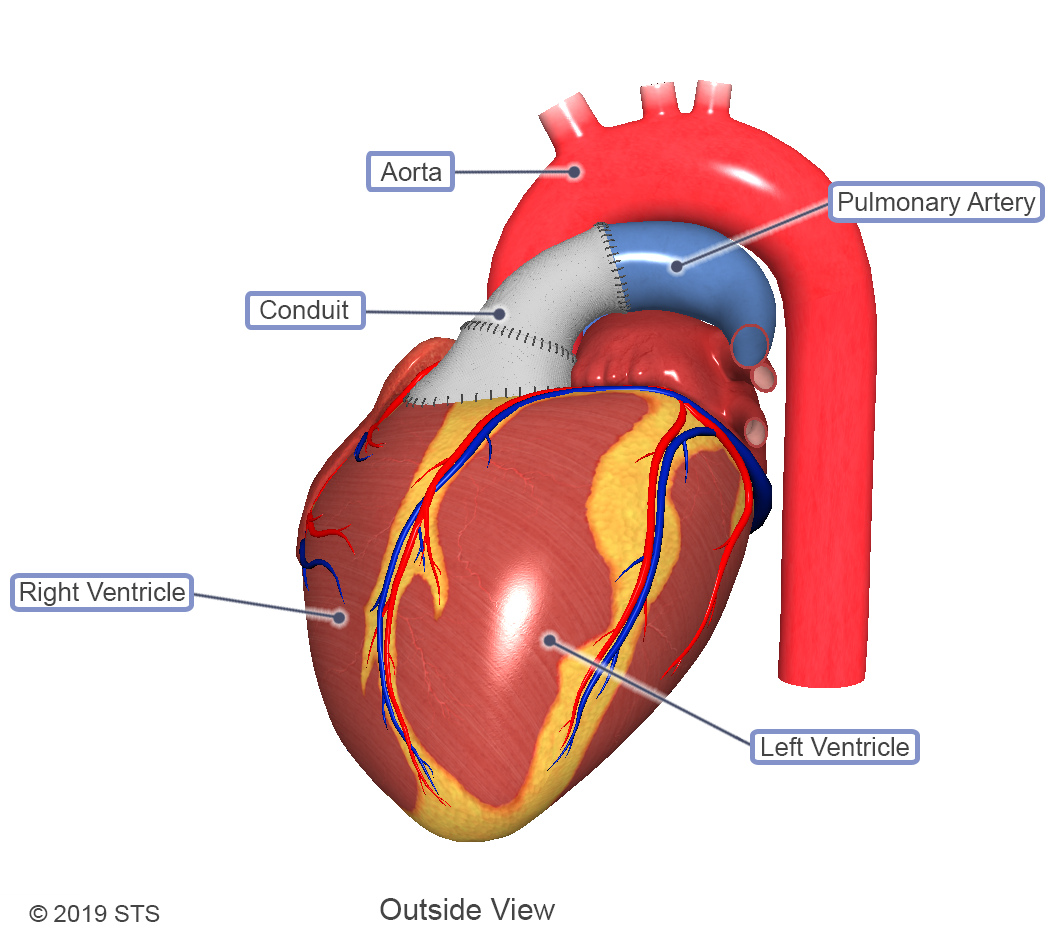
Surgery is the only treatment for truncus arteriosus, which often will be performed before your baby is 3 months old.
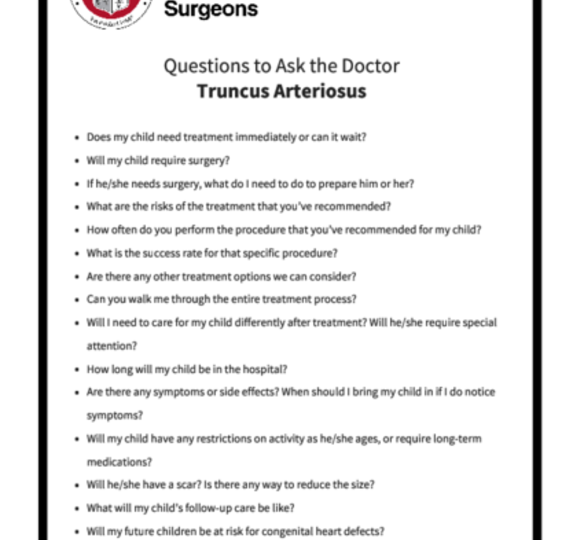
Be sure to speak with your baby’s pediatric/congenital heart surgeon (cardiothoracic surgeon) about what you should expect during and after the surgery. You can print these sample questions to use as a basis for discussion with the doctor.
Expected outcomes: The Society of Thoracic Surgeons (STS) Congenital Heart Surgery Database shows an expected outcome of 6.8% mortality for repair of truncus arteriosus. Outcomes will vary across different programs. It is appropriate to inquire about the outcomes of a surgical group or surgeon during your consultation.
A typical stay in the hospital after surgery is 1 week, if recovery is uncomplicated. If your child needs repair in the first weeks of life, the hospital stay likely will be longer. After repair, most children go on to live healthy, productive lives.

Some children may have restrictions on exercise and certain activities, but speak with your doctor to find out what is recommended for your child.
Your child may be required to take antibiotics during dental procedures to prevent infections that may cause inflammation of the heart (endocarditis). Preventive antibiotics are almost always recommended for people who have artificial valves or who’ve had repair with prosthetic material.
Possible complications later in life include heart failure and having high blood pressure in the lungs (pulmonary hypertension).
Reviewed by: Lauren C. Kane, MD
December 2017
The STS mission is to advance cardiothoracic surgeons’ delivery of the highest quality patient care through collaboration, education, research, and advocacy.