Some babies are born with severe congenital heart defects (present at birth), where the heart is unable to support two separate circulations—one to the lung and the other to the body. Such defects can occur by themselves or as part of certain genetic disorders.
Usually, hearts with congenital defects also have abnormally developed valves and holes between the heart chambers. Frequently, there is narrowing in the tubes (aorta and pulmonary artery) that carry blood out of the heart.
It usually is diagnosed based on the above signs and symptoms, a physical exam, and the results from various tests and procedures.
During a physical exam, your doctor will listen to your baby’s heart and lungs to check for a murmur and will evaluate your baby’s general appearance to look for signs of a heart defect, such as a bluish tint to the skin, lips, or fingernails and rapid breathing.
Single ventricle defects are part of the critical congenital heart defects that can be detected on pulse oximetry. Pulse oximetry is a simple, non-invasive, bedside test to determine the amount of oxygen in the baby’s blood.
If the doctor suspects a single ventricle defect, your baby likely will undergo additional testing. In most cases, an echocardiogram (echo) will provide enough evidence to recommend treatment, but in rare occasions your baby may undergo a cardiac catheterization for further analysis. Additional tests that your doctor may order include a chest x-ray, electrocardiogram (EKG), or magnetic resonance imaging (MRI).
For more information on these tests, visit our common diagnostic tests page.
Currently, no treatment can completely correct single ventricle defects and restore normal circulation.
Over a series of three surgeries, a pediatric/congenital heart surgeon (cardiothoracic surgeon) will “re-route” your baby’s circulation so that oxygen-poor (blue) blood from the body will be diverted directly to the lungs for oxygenation.
This procedure allows blue blood to completely bypass the heart. Oxygen-rich (red) blood from the lungs will return to the heart and the heart will pump this blood to the rest of the body.
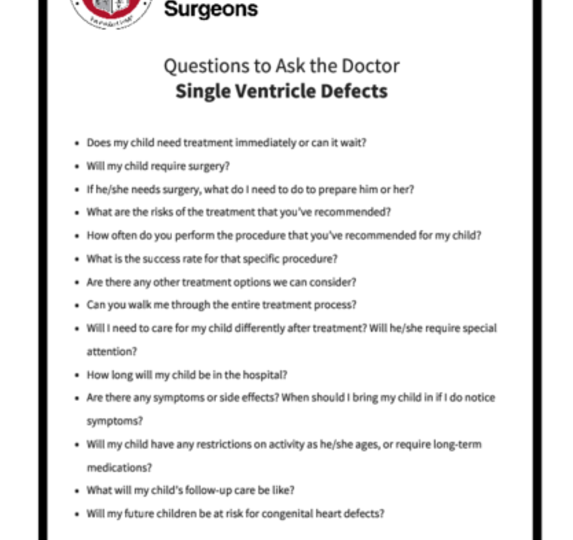
Be sure to speak with your baby’s doctor about what you should expect during and after each of the surgeries. You can print these sample questions (hyperlink to PDF of questions) to use as a basis for discussion with the doctor.
Expected outcomes: The Society of Thoracic Surgeons (STS) Congenital Heart Surgery Database shows an expected outcome ranging from 6.8% mortality to 17.3% mortality, depending on the complexity of the single ventricle palliation surgery. Outcomes will vary across different programs. It is appropriate to inquire about the outcomes of a surgical group or surgeon during your consultation.








The STS mission is to advance cardiothoracic surgeons’ delivery of the highest quality patient care through collaboration, education, research, and advocacy.