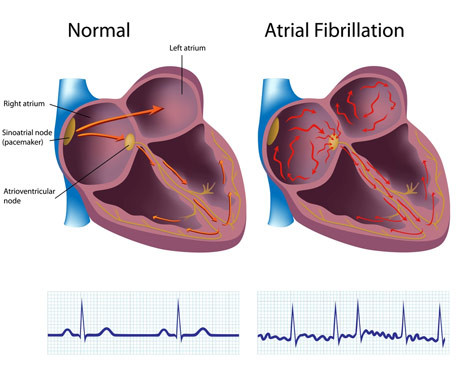
Atrial fibrillation, or Afib, is the most common type of irregular heartbeat (arrhythmia).
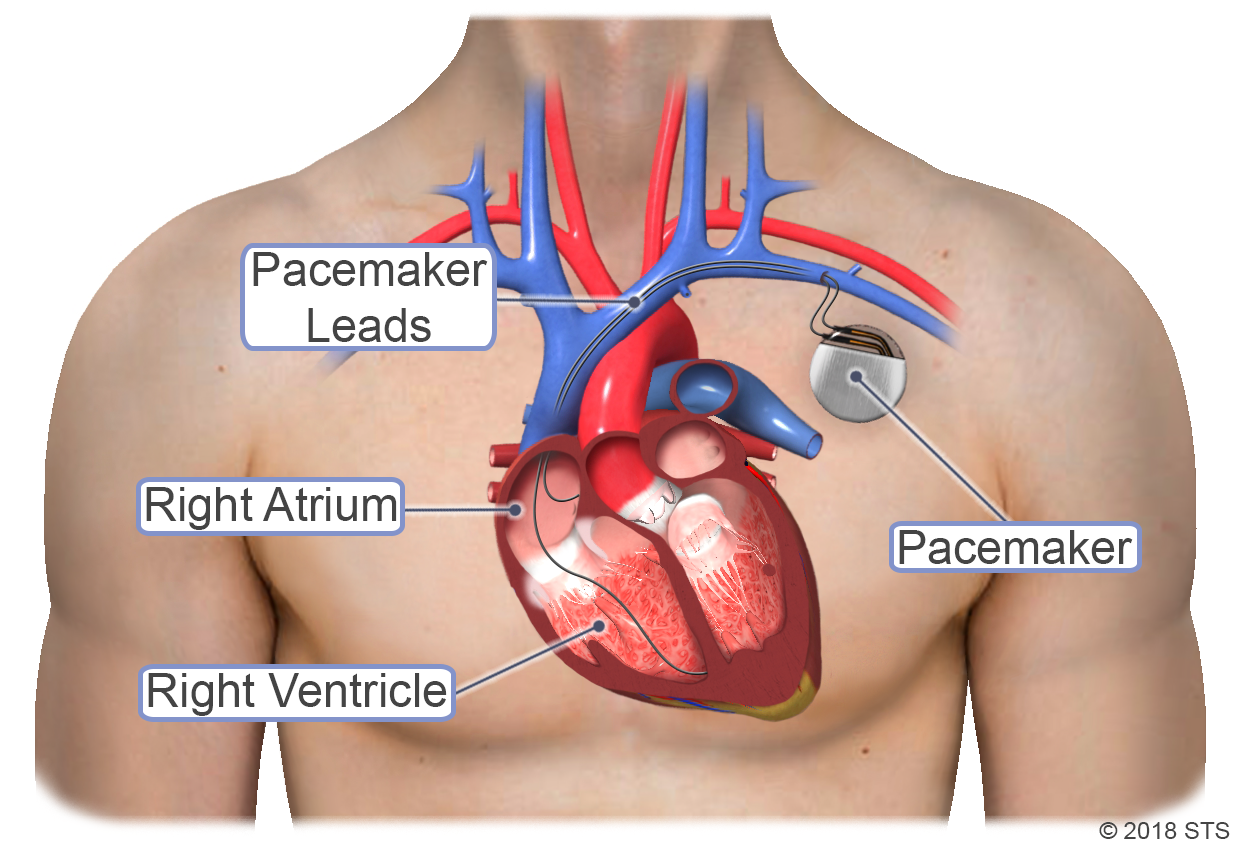
Normally, the upper chambers of your heart (the atria) squeeze first, followed by the bottom part (the ventricles). This contracting and relaxing creates the familiar “lub-dub” beat. The movement pushes blood from the upper heart chambers to the lower ones and out to your body. When you have Afib, the electrical signals that control your heartbeat are out of sync. Instead of working together, the atria quiver or fibrillate; your heart races rather than beats. With Afib, your heart can't pump blood through its chambers and out to your body as well as it should.
According to the American Heart Association, approximately 2.7 million Americans are living with Afib. It is common in people age 60 and older and can lead to blood clots, stroke, heart failure, and other heart-related complications. Untreated Afib doubles the risk of heart-related death and is associated with a 5-fold increased risk for stroke.
The different types of Afib include:
Paroxysmal Afib is when the heart returns to a normal rhythm on its own, or with intervention, within 7 days of when the condition started. This Afib may last for seconds or up to a week before the heart returns to its normal rhythm. Symptoms, which can be mild or severe, are unpredictable and may occur a few times a year or every day. Paroxysmal Afib does not usually require treatment, but often can turn into a permanent form of Afib.
Persistent Afib usually lasts longer than a week. While it may stop on its own, this type of Afib may require medicine or treatment (cardioversion) to help the heart return to normal rhythm.
Long-standing persistent Afib is when your Afib has lasted at least a year without interruption. This Afib can be the most challenging to treat. Medications to maintain a normal heart rate or rhythm are often ineffective. More invasive treatments may be needed to restore your normal heart rhythm.
Permanent (chronic) Afib occurs when the condition lasts indefinitely and cannot be corrected by treatments. This means that your heart is in a state of Afib all the time and that you and your health care team have made a decision not to pursue interventions. However, you may need long-term medication to control your heart rate and lower your risk of stroke.
DIAGNOSIS
If your doctor thinks you have Afib, the first thing he/she probably will do is listen to your heartbeat’s rate and rhythm and take your pulse and blood pressure. The doctor also will ask detailed questions about any symptoms, health habits and problems, and family medical history. Sometimes your primary care or family doctor will be the one who diagnoses Afib. But your doctor also may refer you to a:
- Cardiologist: a doctor who specializes in heart diseases and conditions
- Electrophysiologist: a cardiologist who specializes in arrhythmias
The doctor may order several tests to diagnose your condition, including:
- Electrocardiogram (EKG) is a simple, painless test that records the heart’s electrical activity. It’s the most useful test for diagnosing Afib.
- Holter monitor records the heart’s electrical activity for a full 24- or 48-hour period. You wear this portable EKG device while you do normal daily activities.
- Event recorder is a portable EKG device intended to monitor your heart activity over a few weeks to a few months. You activate it only when you experience symptoms of a fast heart rate.
- Echocardiogram (echo) uses sound waves to create a moving picture of your heart. The test shows the size and shape of your heart and how well your heart chambers and valves are working.
- Transesophageal echocardiography (TEE) uses sound waves to take pictures of your heart through the esophagus. The heart’s upper chambers are deep in your chest and can be seen much better using TEE.
- Stress test puts extra stress on your heart to see how it responds to working hard and beating fast. You’ll be hooked up to an EKG during the test, and the technician will watch your heart rate and blood pressure.
- Blood tests can indicate what may be causing your Afib. Blood tests check for infection, thyroid and kidney problems, and signs of a heart attack.
- Chest X-ray will not show Afib, but it can show complications, such as fluid buildup in the lungs and an enlarged heart.
For more information, visit our common diagnostic tests page.
TREATMENT OPTIONS
Treatment for Afib depends on how often you have symptoms, how severe they are, and whether you already have heart disease. General treatment options include medications, medical procedures, and lifestyle changes. Your doctor will help you decide which treatment is right for you.
The STS mission is to advance cardiothoracic surgeons’ delivery of the highest quality patient care through collaboration, education, research, and advocacy.